YESSSSSSSSSS! I am so glad this day is here! For me, getting a COVID-19 vaccine is like getting into college or getting a new car, it’s such a gamechanger! I am so thankful for TMH getting me in on day 1 in Tallahassee, Florida. And thank you to private industry for finding a solution to the COVID-19 Pandemic.
If you have any doubts about the safety of COVID-19 please read my previous blog posts. As a general pediatrician, I did a lot of reading, and the more I read, the more I wanted a COVID-19 vaccine. Yes, I may get a little soreness or a fever, but THIS IS PART OF THE VACCINE DESIGN. If the vaccine didn’t elicit any inflammation, then the body would not make antibodies against the COVID-19 spike protein.
Hopefully the general public will be vaccinated soon! I did not expect the vaccine to arrive until 2021!!!!!!!!
Blog 4 of the 4 Part Series: Why I Want a COVID-19 mRNA Vaccine (and why you should too).
This is the fourth of four blog posts where I share what I have learned as a Tallahassee pediatrician doing my own research, and why I am excited to receive a COVID-19 vaccine:
Sunday, December the 6th – How vaccines use our immune system to protect us against viruses, bacteria, and even cancer.
Last Wednesday – How mRNA and DNA vaccines are different than traditional vaccines.
Last Saturday – mRNA and DNA vaccine safety in animals and humans.
Today – Post Covid-19 Syndrome
For Young and Middle Age Adults, Post COVID-19 Syndrome May Cause More Suffering Than Acute Symptoms
Even though I turned 40 in 2020 (yes, I know I look 25…except for the hair), I am not as nervous about the immediate effects of COVID-19 (fever, trouble breathing, etc.), as I am about the chronic effects of COVID-19.
Very few people my age actually die from COVID-19, even though many will have flu-like symptoms for over a week or be hospitalized. But now, doctors and scientists are learning that some people will develop chronic COVID-19 symptoms for months, the most common symptom being fatigue, like having Mono, but worse. Others will suffer from shortness of breath, headaches, depression, brain fog, high blood pressure, cholesterol issue, or body aches. Some people alternate feeling fine for a week and then terrible for a week. This diverse group of chronic symptoms has been given the name, “Post COVID-19 Syndrome.”
It would suck to be sick for a few weeks, but it would be even worse to be tired and have body aches for months or years.
Post COVID-19 Syndrome May Be Caused by Damage to Small Blood Vessels
Doctors and scientists are not sure how COVID-19 causes these persistent symptoms, but they think it is from damage to small blood vessels throughout the body–in the heart, lungs, liver, and even the brain. COVID-19’s damage to small blood vessels can cause stroke and heart attacks in relatively young patients (even in patients younger than myself). As you can imagine, blood vessels are found throughout the body, so this may be why the symptoms are so diverse, ranging from depression to trouble breathing.
New Vaccine vs COVID-19 Infection
To me the answer is clear: I would rather take a new(ish) vaccine than get a COVID-19 infection (or a second COVID-19 infection). These new vaccines have already been given to thousands of people without serious side-effects, while we know that COVID-19 can cause death, make you very sick for weeks, and can have long-term side-effects for months and maybe years.
If you are skeptical about the Moderna and Pfizer/BioNTech vaccines, please read my previous posts. The more I learned about them, the more I wanted one!
Blog 3 of the 4 Part Series: Why I Want a COVID-19 mRNA Vaccine (and why you should too).
This is the third of four blog posts where I share what I have learned as a Tallahassee pediatrician doing my own research, and why I am excited to receive a COVID-19 vaccine:
Last Sunday – How vaccines use our immune system to protect us against viruses, bacteria, and even cancer.
Last Wednesday – How mRNA and DNA vaccines are different than traditional vaccines.
Today – mRNA and DNA vaccine safety in animals and humans.
This Wednesday December the 16th – Post Covid-19 Syndrome
The History of mRNA and DNA Vaccines
Starting around 1990, scientists were first able to inject genetic material (mRNA or DNA) into animal muscle AMD get the muscle cells to produce a protein based on this genetic material. This laid the foundation for mRNA and DNA vaccines, which stimulate the muscle cells near the injection to produce the antigen for the vaccine. So far, the biggest challenge with DNA and mRNA vaccines has not been safety but getting them to work. Scientists have continued to tweak the antigen code and the adjuvant effect of the DNA and mRNA. They have also discovered better ways of getting the mRNA or DNA into the cells.
DNA and RNA Vaccines in Humans and Animals
Though the new COVID-19 mRNA and DNA vaccines will be the first fully licensed vaccines for humans, there have been DNA vaccines licensed for animals since 2002. This includes vaccines for fish, dogs, cats, horses, and chickens. None of these licensed vaccines for animals have had to be pulled from the market for safety or efficacy concerns.
mRNA and DNA Vaccines were already in Human Clinical Trials
Starting 10 years before the COVID-19 pandemic, mRNA vaccines had started entering human clinical trials. This includes vaccines against influenza, rabies, cancer, Mono, and Zika virus. In fact, Moderna had already completed a successful Phase 1 Clinical Trial for an mRNA influenza vaccine in 2017. Most of the mRNA vaccines in trials have been safe and effective, but just like traditional antigen plus adjuvant vaccines, some mRNA vaccines were not effective and some had too strong of an immune response. But after a decade of conducting mRNA vaccine trials on thousands of human lives, results have been so good and promising that research and interest has continued to grow.
COVID mRNA Vaccines are 90-95% Effective, in Studies of Over 50,000 People
I am so impressed with reports of 90 to 95% effectiveness. Yes, the Phase 3 Clinical Trials are just finishing, and we only have about 9 months of safety data in humans, but 95% efficacy is awesome! First, many vaccines and medications get to Phase 3 trials just to find out that they do not really work. Second, this is exceeding the CDC’s goal for 70% effectiveness (the seasonal flu vaccine is only 40 to 60% effective every year). 95% Efficacy means that if you give 100 people the COVID-19 mRNA vaccine, and then expose them all to COVID-19, only 5 out of the 100 would contract COVID-19!
COVID mRNA Vaccines have been Safe
So far, COVID mRNA vaccines have been safe. About 1/3rd of people who received the Moderna or Pfizer/BioNTech mRNA vaccines had a reaction. Normally a little redness or swelling at the injection site or mild aches or fatigue. About 2% (2 out of every 100 shots) of study participants had a “grade 3” reaction, which means that the fever, body aches, fatigue, or swelling was severe enough to keep the person from doing his or her normal activities for a day or two. There were no life-threatening “grade 4” reactions in with either mRNA vaccine trial. This is similar to what people experience after a Tdap (tetanus-diptheria-whooping cough) booster vaccine.
What Other Adverse (aka Bad) Reactions were Scientists Worried About?
Some scientists were worried about too strong of an immune response from the adjuvant part of the mRNA. This could have led to high fevers, inflammation, damage of vital organs, or too much swelling at the injection site Thankfully, even though the mRNA immune response has been strong (which is good because it stimulates the body to build antibodies), it has not been dangerously strong. Again, the experience is similar to receiving a Tdap vaccine.
Second, scientists were worried about “Vaccine Enhanced Disease,” where the vaccine makes the real infection worse rather than protecting against the infection. There were some animal vaccine studies of the 2002 SARS Coronavirus (which is similar to COVID-19), in which the experimental vaccine made the SARS infection worse, so scientists were appropriately nervous about VED occurring with COVID-19 vaccination. Thankfully this has not happened. Even when vaccinated people get COVID-19, the COVID-19 infection has been less severe, instead of more severe. More great news!
Third, DNA and mRNA are genetic material. There is a theoretical concern that a DNA or mRNA vaccine could permanently insert foreign genetic material into our DNA, leading to health problems. In the decades of DNA and mRNA vaccine experimentation, this has never happened in animal or human studies (but it could make a good movie).
In conclusion, the COVID-19 mRNA vaccines appear to be very safe and very effective, despite the rapid development and challenges of making a new vaccine. Thankfully, mRNA and DNA vaccines had been in development for decades and were ready to be produced when the COVID-19 Pandemic hit.
I hope after reading this (long) blog, you are encouraged and excited about how our country can overcome this horrible illness. Post with any questions, and read my next blog covering Post Covid-19 Syndrome.
Blog 2 of the 4 Part Series: Why I Want a COVID-19 mRNA Vaccine (and why you should too).
This is the second of four blog posts where I share what I have learned as a pediatrician doing research, and why I am excited to receive a COVID-19 vaccine:
Last Sunday – How vaccines use our immune system to protect us against viruses, bacteria, and even cancer.
Today – How mRNA and DNA vaccines are different than traditional vaccines.
This Saturday – mRNA and DNA vaccine safety in animals and humans.
Wednesday December the 16th – Post Covid-19 Syndrome
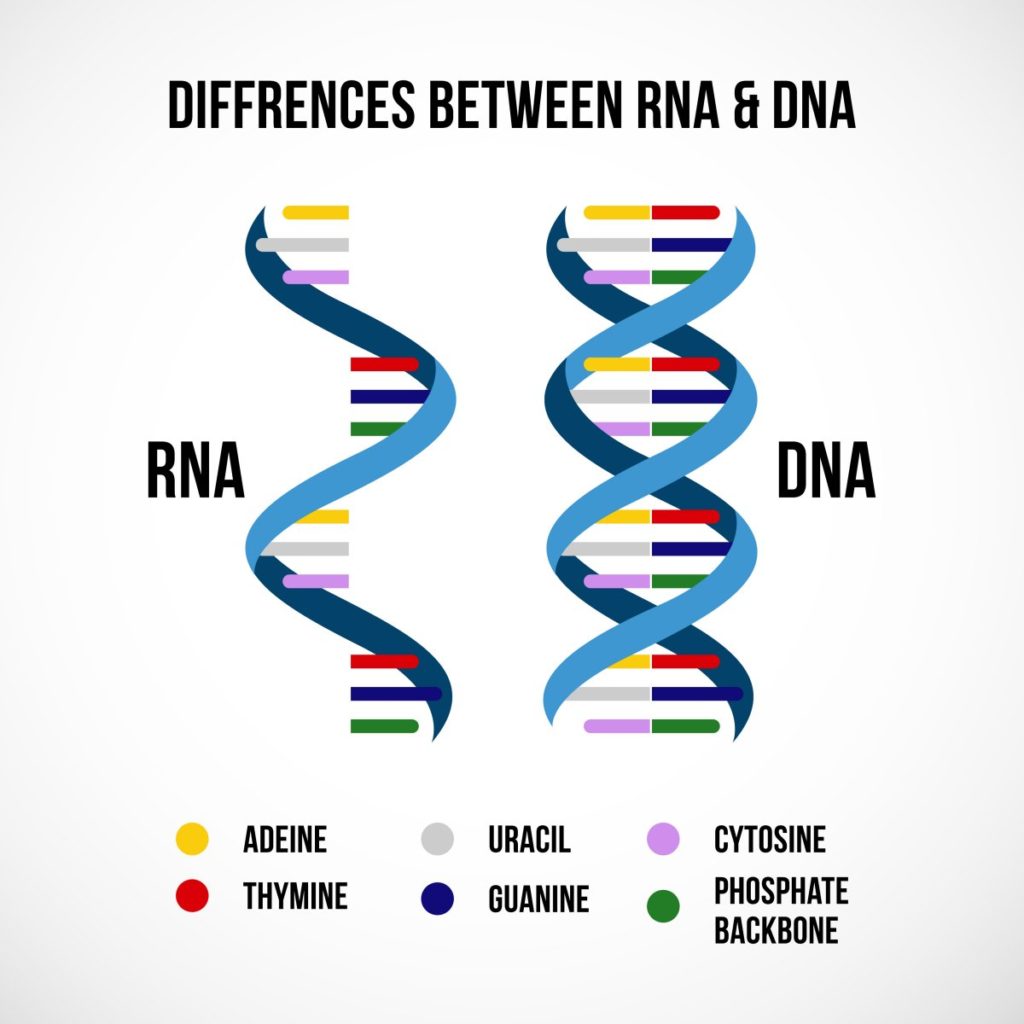
What is the Difference Between mRNA and DNA?
Our genetic code is stored in a DNA “double-stranded” spiraling helix, made-up of 4 different DeoxyriboNucleic Acids, corresponding to the A, T, G, or C of our genetic code. Think of DNA as our genetic code storage facility, and RNA (RiboNucleic Acid) as genetic copies that your body uses to make and do things. RNA copies that are used to build things are called “messenger RNA” or mRNA.
Why Use mRNA (or DNA) in Vaccines if all You Need is an Antigen and an Adjuvant?
In my first post, I explained how a vaccine basically has two parts: an “antigen” (for COVID-19, usually the “spike” protein) and an “adjuvant” to stimulate the immune system. Traditionally, vaccine companies make large quantities antigens and adjuvants and then package them into small vials for use. In fact, 5 of the 11 COVID-19 vaccines in clinical trials are being produced just like this. The problem is that takes a lot of time and money to design and build the manufacturing plants that safely and efficiently produce the antigen and adjuvant for a vaccine.
Alternatively, mRNA vaccines (and DNA vaccines) use our own human cells’ built-in protein making ability. The mRNA (or DNA) stimulates our own cells to make the antigen! So instead of having to manufacture a new adjuvant and antigen for every new vaccine, scientists can simply alter the mRNA (or DNA) code so that a different antigen is produced by the cell. And as an added bonus, RNA and DNA generally do not need added adjuvants, as they have built-in genetic code that triggers an immune response.
mRNA and DNA Vaccines Stimulate Cells to Make Antigens and Stimulate the Immune System to Make Antibodies.
In Summary, the mRNA in COVID-19 mRNA vaccines both stimulates human cells to make the COVID-19 spike protein AND stimulates the immune system to make antibodies against the COVID-19 spike protein. This saves both time and money, because scientists and engineers do not have to design and build manufacturing plants to produce large quantities of antigen and adjuvant. Instead, scientists can simply change the mRNA in a mostly ready-to-go system to rapidly manufacture a new vaccine.
In my next post this Saturday, I will review this history and safety of both human and animal mRNA and DNA vaccines. There will be a lot of good information! For example, did you know DNA vaccines have been licensed for use in animals since 2002?
Like most of you, I have been encouraged by reports of 90% efficacy of both the Moderna and Pfizer/BioNTech mRNA vaccines. After all the human suffering from COVID-19, it would be great to end the pandemic with a human success story. Distribution of the vaccines could start next month in the U.S. and maybe next week in England.
And I will be the first in line to receive the vaccine! I was initially nervous about receiving and recommending a vaccine made with new technology against a new virus. But, I’ve done my research, and I really want to get one of these new vaccines.
This is the first of four blog posts where I share what I have learned, and why I am excited to receive a COVID-19 vaccine:
Today – How vaccines use our immune system to protect us against viruses, bacteria, and even cancer.
Wednesday – How mRNA and DNA vaccines are different than traditional vaccines.
This Saturday – mRNA and DNA vaccine safety in animals and humans.
Wednesday the 16th – Post Covid-19 Syndrome
Part 1: How Vaccines Use Our Immune System to Protect Us Against Viruses, Bacteria, and Even Cancer
Our Immune System is Constantly Exposed to “Antigens”
Our body is constantly exposed to foreign material, which scientists call “antigens.” Every day, THOUSANDS of antigens make it into our body through the air we breathe and the food we eat. Our immune system is alwasy on the look-out for these foreign antigens, because some are dangerous (live viruses, bacteria, parasites, and cancer). Most of the time these antigens are harmless. They are quietly recognized and gobbled-up by our immune cells, not creating any noticeable immune response.
Our Immune System Makes Antibodies Against Dangerous Antigens
But sometimes an antigen will begin to damage cells in our body (like bacteria damaging your skin). The damaged cells send out alarm signals to the immune system. These alarm signals do many things, one of which is to activate the “humoral immune system,” which produces “antibodies” to this new, dangerous antigen. Antibodies are small proteins that float around in our blood (and the lining of our lungs and GI tract) that are custom made to stick to a specific antigen. If effective antibodies are produced to an antigen, the next time this dangerous antigen enters the body, these antibodies will quickly stick to the antigen and label it as dangerous This will trigger the immune system alarms, so that the antigen can be quickly destroyed before it damages too many cells (like it did the first time).
Vaccines Contain an Antigen, Designed to Make Antibodies
A vaccine basically puts a safe antigen into body, which stimulates the immune system to make effective antibodies against a dangerous disease (like COVID-19). It sounds simple, but there are many challenges to making an effective vaccine to a new virus. First, scientists had to decide which part of the virus to use as the antigen. Remember, the antibodies produced by the antigen would have to work against the real COVID-19 virus. Many experimental vaccines fail because they don’t create effective antibodies. And, you can’t just use the whole live virus as the antigen, or the virus will make people sick! Thankfully, scientists had already learned from previous Pandemic Coronaviruses that antibodies against the “spike” protein of the virus’s fatty cover seemed to work, and they already had experience making a spike protein antigen.
Scientists Must Use the Right Adjuvant to Stimulate the Immune System
But, if you inject someone with the spike protein alone, it probably won’t cause any damage (since it’s just one part of the virus), and it will just be gobbled-up by our immune system without producing any antibodies. So scientists must also include an “adjuvant” along with the spike antigen, that “tricks” the immune system into thinking that the spike antigen is dangerous and therefore the stimulating the immune system to turn on the alarms and make antibodies against the spike protein. Adjuvants are made of many compounds, including synthetic DNA resembling bacteria DNA, aluminum, and even proteins from the Chilean soapbark tree that the immune system thinks are dangerous bacterial proteins.
It Takes Time to Manufacture Safe Antigen and Adjuvant
So, at the most basic level, a vaccine is composed of both an antigen that can be used to make effective antibodies, and an adjuvant that stimulates the immune system to make antibodies. In fact, five of the eleven COVID-19 vaccines in stage 3 clinical trials are simply antigen-adjuvant vaccines. In my next blog, I’ll explain how mRNA and DNA are different (spoiler alert—they get our own cells to make the antigen).
Leon County schools restart this Monday, and as a pediatrician in Tallahassee, I am hearing than many children (and parents) are feeling the grip of anxiety. With so many changes, such as masks and new drop-off rules, it is appropriate to feel some level of anxiety. Here are a few tips to cope with the new changes and the new school year:
1. Talk to your child about the changes
If you haven’t already, talk to your child about the changes. Younger children (like elementary school) will need these in more concrete terms, while older elementary, middle, and high school children may want to discuss topics more deeply. Sometimes this discussion is easier over a snack or a meal.
For example, you might say to your first grader, “School is starting tomorrow. You are going to get to see friends and your new teacher. School is going to be a little different this year. Teachers and kids will be wearing masks, and you will need to have your temperature checked every morning, but after a few days, the new changes will start to feel normal. What do you think about that?”
(It is sad for our kids that this will be the new normal for a time.)
For younger kids, give them the facts, and then wait and see how much more they want to know (if any).
2. Validate worries
It is totally appropriate to feel anxiety about this new school year as there are so many changes. If your child expresses worries about the new year, validate their concerns before telling them they will be okay.
To a first grader, you could say, “Jennifer, you are right. It is normal to feel sad that your best friend won’t be at school this year. But you know what? We will try to arrange playdates with her outside, AND remember all the new friends you made last year at school?”
3. Plan some special rewards
Looking forward to something special after school can help your child make it through the day. Consider rewarding your child for the first few days of school with a joint activity that includes one-on-one parent time. Examples are baking, doing a puzzle, playing chess, exercising, or going out for ice cream.
4. Practice anxiety-forming activities
If your child voices concerns about new procedures, such as getting his or her temperature checked or school drop-off, then practice these with your child. Practice should be just playing a make-believe or pretend game.
For example, if you child is nervous about getting her temperature checked everyday, explain to him or her how it will happen. Then ask your child who would they like to be, the adult or the child? Then act it out a few times, maybe even trading places. You can do the same for school drop-offs and walking into the classroom.
5. Contact your school’s guidance counselor and/or pediatrician
If you have spoken to your child and practiced everything, and the anxiety or fear is just overwhelming, then I recommend speaking to your school’s guidance counselor or pediatrician for more help. Most schools can make exemptions for children who are significantly affected by anxiety. For example, the school may be able to provide a consistent person for car drop-off. Sometimes it may help to have a note or a call from your child’s pediatrician.
In general, going back to school is going to be beneficial for so many kids. The lack of social interaction has been very hard on children and their families. But for many kids, Monday is going to be a tough day. Some kids will not make it out of the car, AND THAT IS OKAY, just make sure and contact your school’s counselor and/or your pediatrician.
Good luck everyone! Message me with questions or comments!
Dangerous websites, such as pornography, are just one Google search away from our children.
The exponential increase in children opting for virtual school will give children unsupervised access to the internet like we have never seen before. The computers that they will be using to access virtual classes and homework, give anyone access to anything on the internet.
And parents, including myself, don’t think that our eleven year-old would ever start looking at pornography. I mean, where would he or she get the idea? How would they know what to search for? And wouldn’t I find out?
But let me tell you, as a pediatrician and the parent of tweens, our kids are finding this stuff. In the exam room, many teenagers have confidentially shared what they have seen and watched online–and it’s not healthy. And not just teenagers but preteens as well!
And online pornography is dangerous for the mental health of our children, much like the pornographic magazines of the 80’s and 90’s, but even more so. There are many harmful effects of pornography on the childhood brain, and I will briefly review two here:
Online Pornography is Unhealthy
First, like a drug, Online Pornography is Addictive
Online pornography acts like a drug on our brain. Online porn scenes cause rapid and high levels of dopamine to be released into the brain. And just like a drug, teens who engage in online pornography will want more and more exposure to more and more provocative images, to experience this rapid and high level of dopamine release into the brain. This can lead teens to “waste time” on their computer, spend less time with their friends, and become lonely and depressed.
And recent research has shown that this effect is more pronounced on the teenage brain!
Second, Online Pornography can lead to Sexual Dysfunction
As adults, we know that pornography scenes are staged and fake, but children will take what they see as normal. This can lead to unhealthy expectations in their sexual encounters and can also lead to sexual dysfunction. And as “addicted” children watch more and more graphic pornography, they will have trouble with “normal” sexual function in a “normal” encounter.
What Can You Do? “CPR”
There is no perfect solution. If not at our own home, our kids may be exposed to dangerous websites at a friend’s home or on a friend’s device. But the best strategy consists of three tiered approach I call “CPR”:
Communicate with your child about the dangers of the internet.
Physically monitor potentially dangerous internet use.
Restrict internet or device access to dangerous websites.
1. Communicate with your child about the dangers of the internet.
This is just like other important conversations that we will have with our children: sex, drugs, alcohol, and now add the internet. Depending on your children, around 9 to 11 years of age, I recommend sharing your views on the good and bad of the internet with your child. And if you don’t know what you believe, do some research. Read about how pornography, screen time, meeting strangers, etc. can all affect your child.
2. Physically monitor potentially dangerous internet use.
Most of the time, you can restrict your home internet or your child’s device from having internet browser (Chrome, Edge, Firefox, etc) access, but sometimes you can’t. If your child needs to access his virtual classes through a browser, then you have no choice but to allow internet browser access. But, you only need to allow them access to this device as necessary, and try to physically monitor what they are looking at. You cannot be there 100% of the time, but make sure that their device or computer is in a public area where you or other family members can easily see what they are doing. I strongly recommend against allowing a child to have internet browser access alone in their room.
3. Restrict internet or device access to internet browsers
It is much harder on computers and still very difficult on tablets and phones, but try to use parental monitoring software, like Apple’s Screentime, Google’s FamilyLink, or Disney’s MyCircle to completely block browser access. For example, with Apple’s Screentime, you can choose what apps your child has access to. If you really feel like they should be able to “browse” the internet, you can download child-friendly apps and browsers that allow you “whitelist” only certain websites that your child can visit.
Life with tech is tough
Technology has made our life better in so many ways, but it has definitely made it difficult to keep our children from being exposed to harmful material. Our parents had to make sure we didn’t have Showtime or HBO access as kids, but the internet is a whole new monster. And now that thousands of children will be spending thousands of hours online, we parents need to be proactive and protect our children. Our tween and teens will put up a fuss, but we need to do what is best for them.
Advocate for Change
One last thing we can do is advocate for our children. Ask your teachers and schools to include all their material in one internet location. For example, if a teacher requires a student to watch a video on YouTube, then you must leave YouTube unblocked, and your child will have access to anything on YouTube. But, if your school places all of their educational material on their own website or portal, then you can restrict YouTube access, protecting your child from potentially harmful material.
After a double-length summer, many kids are going to have trouble staying focused in class (or at home)! As a pediatrician, I know that many children already had trouble focusing in the classroom, and now parents are telling me that they are having even more trouble at home. So, given the popularity of my last post “Vitamins That Boost Your Immune System,” I am sharing safe and effective doses of supplements that boost your child’s focus and attention. This is the same information I share with my parents in my Tallahassee pediatric office, Canopy Pediatrics.
Omega Fatty Acids – total milligrams (mg) per day of DHA, EPA, and ALA
Age
Starting Supplement
Maximum Supplement
2-4
500mg
*speak to your pediatrician
5-9
750-1000mg
*speak to your pediatrician
10+
750-1000mg
2000mg
The supplement should consist mostly of DHA and EPA with about 10% ALA. Some studies have shown improvement without ALA supplementation.
The omega 3 fatty acids, DHA and EPA, are the most effective supplements to improve focus and attention. Studies have show that even some children diagnosed with ADHD show modest benefits with proper omega 3 fatty acid supplementation. In addition to an improvement in focus, DHA and EPA can improve oppositional (or uncooperative) behavior and emotional lability (getting sad or upset easily) in children as well. There is even some evidence it can help a depressed mood.
The omega 3 fatty acid ALA is the most common in the American diet, and the body can make DHA and EPA from ALA, just not very well. This is why most of supplementation is in the DHA and EPA form.
Most studies of omega 3 fatty acids in children use a dose between 750 and 1000mg per day. One downside of omega 3 fatty acid supplementation is that it can take up to three months to show an improvement, so don’t give up too early! I recommend the starting doses in the chart above. If your child is age 10 or older, and the starting dose is not effective after 3 months, then you may increase the dose, just stay under 2000mg per day.
Zinc – in milligrams (mg) per day
Age
Recommended
Maximum
Supplement
1-3
3
7
3
4-8
5
12
5
9-13
8
23
10
14-18
9,11*
34
20
19+
8,11*
40
25
*males 14 and older require more daily Zinc than females
Zinc is another supplement that has helped children with focus and attention. In one of my favorite studies, American children with ADHD supplemented with Zinc used 30% less Ritalin to control their symptoms. If Zinc is good can help children with ADHD, then it can help “normal” children stay focused–in addition to helping the immune system!
Melatonin and Sleep
Getting plenty of sleep is important for focus and attention. Some children may not be focusing well, because they are not getting enough sleep or good quality sleep! These children may have a medical reason for poor sleep (such as large tonsils or adenoids), or they may have poor “sleep hygiene” (using electronics too late, leaving a TV on all night, drinking caffeine in the evening, etc.). These children first need to be evaluated for medical causes of poor sleep. If no medical reasons are found and sleep hygiene has been addressed, then talk to your pediatrician about melatonin supplementation.
More Help
Many children need more than supplements to improve their focus. I approach focus and attention problems holistically: I examine the child’s diet, sleep, school performance, and environment. And before jumping straight to medications (which are important for many children), I suggest a variety of natural and safe alternatives. Contact my office for a free consultation!
As a pediatrician in Tallahassee, Florida, I have been supplementing my immune system with three vitamins, Zinc, Vitamin D, and Vitamin C since the COVID-19 Pandemic began. I wanted to do everything I could to keep myself well for my pediatric patients at Canopy Pediatrics.
Our children in Tallahassee will be returning to school soon, and they WILL be exposed to COVID-19. Prepare your child’s immune system with the same vitamins that I have been taking. The far right columns below contain a safe amount of vitamin that you can use to supplement your child.
My suggested supplementation is a little less than the difference between the National Institute of Health’s maximum intake and the recommended intake (RDA) for each vitamin. To be safe, you do not want to go over the maximum daily amount, as even vitamins can be harmful. I do not recommend simply supplementing with the maximum daily amount, as many American children already get the recommended daily amount of each vitamin through their diet (so supplementing with the maximum amount would give them more than the daily maximum).
Zinc – in milligrams (mg) per day
Age
Recommended
Maximum
Supplement
1-3
3
7
3
4-8
5
12
5
9-13
8
23
10
14-18
9,11*
34
20
19+
8,11*
40
25
*males 14 and older require more daily Zinc than females
Besides boosting the immune system, Zinc is important for wound healing and focus. The best natural sources of Zinc are shellfish (especially oysters), meat, legumes, and cheese.
Vitamin C – in milligrams (mg) per day
Age
Recommended
Maximum
Supplement
1-3
15
400
200 – 300
4-8
25
650
400 – 600
9-13
45
1,200
500 – 1,000
14-18
65,75*
1,800
1,000 – 1,500
19+
75,90*
2,000
1,000 – 1,500
*males 14 and older require more daily Vitamin C than females
Although people who supplement with Vitamin C still catch viral infections (like COVID-19) their symptoms are milder and last a shorter amount of time. Besides boosting the immune sytstem, Vitamin C my also prevent cancer and cardiovascular disease. The best natural sources of Vitamin C are citrus fruits, kiwi fruit, strawberries, cantaloupe, tomatoes, and broccoli. Also, check labels, as it is added to many packaged goods and beverages.
Vitamin D – in international units (IU) per day
Age
Recommended
Maximum
Supplement
1-3
600
2,500
1,000 – 1,500
4-8
600
3,000
1,000 – 2,000
9-13
600
4,000
2,000 – 3,000
14-18
600
4,000
2,000 – 3,000
19+
600, 800*
4,000
2,000 – 3,000
* people 70 years of age and older require more daily Vitamin D
Some research has shown a correlation between vitamin D deficiency and severe COVID-19 illness, and there an ongoing study investigating whether vitamin D supplementation at the time of COVID-19 diagnosis can reduce the severity of symptoms.
As a pediatrician, I sometimes screen children for vitamin D deficiency, and I am always surprised how many kids are deficient. I suggest not waiting, but rather start supplementing with vitamin D now. The best natural source of vitamin D is sunlight, and people don’t need much sunlight to meet requirements. 5 to 30 minutes (depending on your skin color, as lighter people need less sun, and sun brightness) of sunlight exposure twice per week is usually enough for someone to meet their requirement of vitamin D. Vitamin D is also added to most cow and vegetarian (soy, almond, etc) milk.
In addition to supplementing with vitamins, I have tried to be more consistent with my exercise, as COVID-19 frequently causes lung infections (aka pneumonia). So, don’t forget that children aged 5–17 should get at least 60 minutes of moderate-to-vigorous physical activity every day (my children often complain, but think of it as good medicine!).
Leave a comment with any questions or suggestions!
As a pediatrician in Tallahassee, Florida, I have only seen a few cases of Coronavirus in children. I have had no cases of COVID-19 in my pediatric office, Canopy Pediatrics, and until the last few days, I had only seen a handful of COVID-19 cases while working in the pediatric ER for Capital Regional Medical Center (and these were mostly teenagers). Only one child was ill enough to warrant a hospital admission, and this child probably had a severe complication of COVID-19 in children called “Multisystem Inflammatory Syndrome in Children,” (MIS-C) which I will discuss further below. Since I am gathering information for an interview with WTXL TV to discuss how children are affected by COVID-19, I decided to share what I’ve learned here:
First, let me paint an overall picture of the medical effects of COVID-19 on children. Like adults, children infected with COVID-19 experience “flu-like” symptoms (some or all of the following): fever, cough, sore throat, congestion, runny nose, body aches, and sometimes vomiting, diarrhea, and abdominal pain. Sometimes they can develop a rash.
So far, COVID-19 infections in children seem to be less common, less severe, and less contagious in children than in adults. I say “seem” for two reasons: First, compared to adults, children have been much more socially isolated than adults (for example, most schools have been closed since March, but many adults have continued working or going to the grocery store), so better social isolation than adults is definitely one contributing factor to fewer kids being infected with COVID-19. Second, new information is always being discovered about how children are affected by COVID-19 in children.
Children Have Less Severe Infection
Regarding severity, reviews of children have found that about 15% of COVID-19 infected kids will be asymptomatic and 80% will have some mix fever, cough, and congestion without a low oxygen level (Flu-like symptoms), and less than 1% will need to be hospitalized. Compare this to adults, where 1% of adults aged 20-49, about 5% of adults aged 50-59, and 18% of adults over 80 years-of-age infected with COVID-19 will require hospitalization. So, kids generally do pretty well with COVID-19.
But, even though the average child has a less severe COVID-19 infection, very rarely, in about 1 in 300 COVID-19 pediatric cases, a syndrome occurs called “Multisystem Inflammatory Syndrome in Children” (MIS-C). MIS-C usually occurs 1 to 3 weeks after the onset of the child’s COVID-19 illness or can even occur after an asymptomatic infection. I hope MIS-C does truly occurs in 1 in 300 children infected with COVID-19, because for me personally, it has happened in 1 of about 10 children that I have seen with COVID-19. As the name implies, many systems of the body are severely affected. Symptoms include high and prolonged fevers; headache, confusion, or seizures; heart abnormalities; abdominal pain, vomiting, or diarrhea; and skin rashes, sore throat, and pink eye. And to make matters worse, most of these children have negative nasal swabs for COVID-19, but have positive COVID-19 antibody blood tests, meaning that MIS-C usually occurs as a complication towards the end or after an infection with COVID-19. Treatment for MIS-C is currently under investigation.
Children Seem Less Contagious
Children (especially prepubertal children) seem to be less contagious and become infected less often than adults. Children of all ages can still get a serious COVID-19 infection, but most of the evidence points to children generally being less contagious. In studies, young children (less than 10 to 12 years of age) have been less likely than adults to catch Coronavirus whether they are at home, at school, or just living life. On the other hand, teenagers with Coronavirus are probably just as contagious as adults and just as likely to catch the disease. Much of this information comes from comparing high schools, middle schools, and elementary schools in the same town and by looking at whom gets infected in a household.
There have been recent stories of outbreaks among children at camps, especially overnight camps. This reiterates that even if everything is done correctly, many children will still become infected with COVID-19. But it also reiterates that given the right (wrong) circumstances, like singing in groups or sleeping in a one room cabin with teenage counselors, COVID-19 will quickly spread from child to child.
Additionally, on July 30th, in a JAMA Pediatrics article, investigators found higher levels of COVID-19 viral RNA in children’s nostrils compared to COVID-19 positive adult noses. The clinical significance of this finding is yet to be seen. Many pediatricians think that since kids are not getting tested as much as adults (as many COVID testing sites will not test kids), the children in this study might have been more sick than the adults.
Why Are Children Less Affected?
So why is COVID-19 generally less severe in children than adults? Scientists are considering a few possibilities. One is that nasal tissue of younger children (less than 10 years of age) have less of the “ACE2” receptors that COVID-19 uses to enter into cells. A second possibility is that children have a less intense full body inflammatory response than adults. A third possibility is that children commonly co-infected with other viruses, and maybe other viruses are “running interference” leading to less COVID-19 virus production. And a fourth possibility is simply that children have relatively healthier blood vessels than adults.
How Are Different Ages Affected?
So, how are different ages of children affected? First, it does appear that children under 1 year-of-age, particular infants less than 3 months-of-age, are more susceptible to the effects of COVID-19 than older children. A few studies have shown an increased hospitalization rate in this age group. Also babies with Coronavirus may not have the typical fever, cough, and congestion of older children, but rather may present with trouble eating or fussiness.
Now the safest age to be right now is between 1 and 10 years of age. Many studies have shown that this age group is the least likely to get infected when exposed to COVID-19, the least likely to have serious illness from COVID-19, and the least likely to spread COVID-19 if infected. This may be because this age group has less ACE2 receptors than adults AND has a stronger body and immune system than an infant. But it is this age group that generally gets the severe MIS-C.
There is still some question as to whether kids over the age of 10 (tweens and teenagers) are less susceptible to COVID-19 than young and middle-aged adults. A few large studies, where large groups of people were swabbed, found similar rates of COVID infection in children 10-18 as adults. But, studies do show that teenagers are hospitalized less often than young adults. This could simply be that teenagers are less obese and have less chronic conditions than young adults.
So practically what does this mean?
First, for parents of infants or are pregnant: COVID-19 is more dangerous in babies than older children, so these parents should be extra careful to limit potential exposure to COVID-19, especially during the first three months of a baby’s life. These families should limit visitors and require that all visitors self-quarantine for 14 days before spending time with the baby. They can also limit the infant’s exposure to COVID-19 by finding a pediatrician who allows families to wait in the car (rather than a waiting room) or who provides home visits.
Second, for social interaction outside of school: Children, and their parents, are going crazy, not being able to interact with their friends and family. I think this data supports the idea that occasional close social interactions between toddlers or school-aged children (prepubertal kids) of different families (whose parents are otherwise being careful to social distance and do not have chronic conditions themselves), may be worth the risk for some families (as long as the parents keep their distance from each other). For many families, the low (but still substantial) risk of infection may be worth the trade-off for quality social interaction for their children. But again, the parents would need to practice good social distancing, so that they don’t accidentally infect each other.
On the other hand, close social interaction between kids over the age of 10 is more risky, which is too bad, because this is the age group that really needs social interaction. If kids of this age get infected, they will most likely do well themselves, but they are at high risk of passing the infection to siblings, parents, or other friends, which will lead to worsening of the COVID-19 outbreak.
And last, there is always the risk of a child developing COVID-19 Multisystem Inflammatory Syndrome in Children (MIS-C). As I mentioned earlier, scientists think it only occurs in 1 in 300 children infected with COVID-19, so hopefully my experience with MIS-C will not be the norm.
How Can Families Medically Prepare?
To be ready for this fall and winter, families need to have a pediatrician or family doctor that they can easily reach, and that they trust. When a child develops symptoms of a possible COVID-19 infection, this first thing to do is call or text your primary care physician for guidance.
And families can rest assured that Tallahassee has great emergency rooms and hospitals, like CRMC and TMH, that are prepared to evaluate their child in case of severe or concerning symptoms.